









Metatarsal Fracture
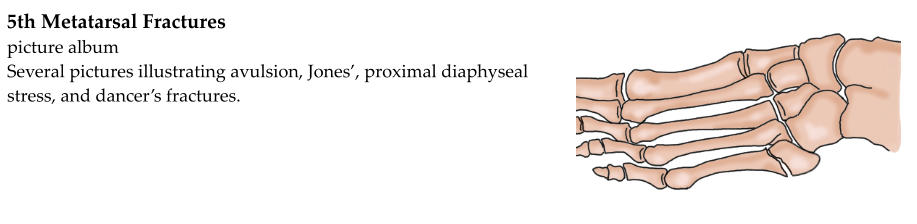
The long bones of the foot are called the metatarsals. There are 5 metatarsals -- one for each toe. An injury to the
foot can break one or more of the metatarsals. This is known as a metatarsal fracture.
Metatarsal fractures often occur as the result of “rolling” or twisting the foot. They may also occur with a
traumatic blow, such as dropping a heavy object on the foot. Some metatarsal fractures are stress fractures. This
means that the fracture does not occur as the result of one specific injury. Instead, repetitive blows to the
metatarsal, such as the foot pounding the ground while running, gradually overload the bone and cause it to crack.
Metatarsal fractures may involve the head, neck, shaft, or base of the metatarsal.
Metatarsal fractures are diagnosed based on a history, physical exam, and x-rays. Patients usually report twisting
the foot or sustaining a traumatic blow. If they have a stress fracture, they may report gradually worsening pain,
especially with running or strenuous activity.
Upon physical exam, the foot may be bruised and swollen. The broken bone will, of course, be tender to push on.
X-rays are important not only to confirm that the foot is broken, but to evaluate the fracture. Fractures may be
non-displaced (just a crack) or displaced. They may involve the cartilage in the joints (intra-articular). They may
be angulated (bent at the fracture site). Certain locations in the metatarsals are known to have an unreliable blood
supply, and may not heal as well.
Non-displaced metatarsal fractures can be treated without surgery. A cast, boot, or hard-soled shoe is applied for
4-6 weeks. Depending on the location of the fracture, weightbearing may or may not be permitted. Follow-up x-
rays are obtained to evaluate healing.
If the metatarsal fracture is displaced or angulated, it may require surgery. Fractures with a little bit of angulation
to the side may not need surgery, but fractures with angulation in the plantar or dorsal direction (up and down)
need to be corrected.
Stress fractures may or may not be visible on x-rays. If a stress fracture is suspected by not visualized on an x-ray,
an MRI or bone scan may be obtained.
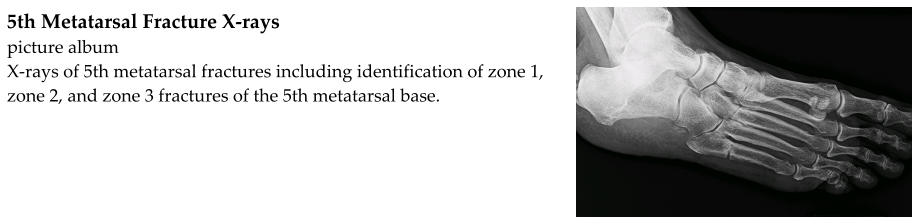
Fractures at the base of the 5th metatarsal (the bone on the outer side of the foot) are a special case. The blood
flow to the 5th metatarsal base is unusual. Good blood supply is important for fracture healing. Some 5th
metatarsal fractures do not heal as well. These fractures may be treated more aggressively with casting and non-
weightbearing or surgery.
If surgery is needed, the fracture is reduced (the bone fragments are pushed back into place) and then pins,
screws, or plates are used to hold the fragments in place while the fracture heals. Sometimes the fracture can be
pushed back into place without making an incision. A pin can then be pushed through the skin and drilled into the
bone. This is known as percutaneous pin fixation or closed reduction-internal fixation (CRIF). Pins are often
removed in the office a few weeks later. Sometimes the fracture cannot be successfully reduced without making
an incision and exposing the bone. This is known as open reduction-internal fixation (ORIF). Screws or plates
may be used to fix the fragments in place. These are generally not removed.