









Ankle Sprain
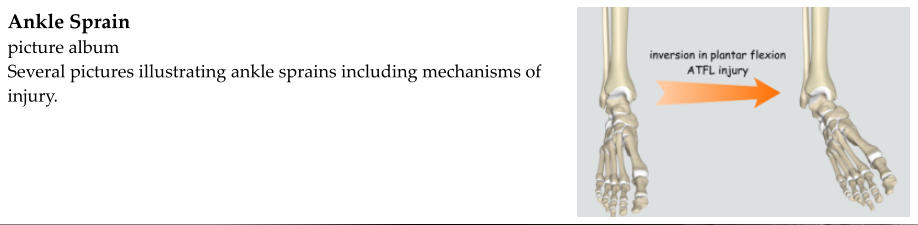
Injuring the ankle in such a way as to stretch or tear one or more of the ligaments that stabilize the
ankle joint is referred to as an ankle sprain.
Very common
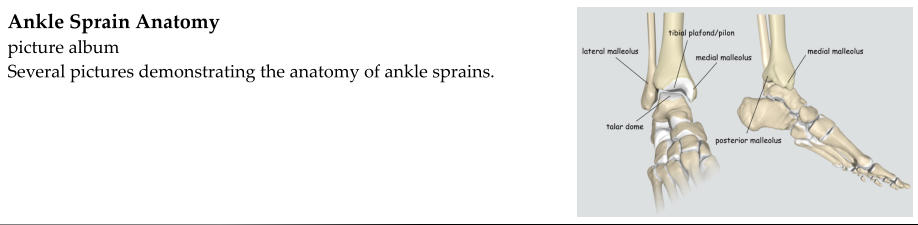
The ankle joint is formed where the fibula, tibia, talus, and calcaneus come together. The lateral
malleolus of the fibula and the medial malleolus of the tibia form a mortise in which the talus sits. The
talus rests on top of the calcaneus.
Ligaments are strong bands of tissue that hold bones together. There are several ligaments that hold
the bones of the ankle together.
Symptoms:
•
Ankle pain after a twisting or “rolling” injury
•
Ankle swelling, bruising
Physical exam:
•
Swelling, bruising of the ankle
•
Ankle tenderness, especially over the injured ligament(s)
•
Anterior drawer - assess for instability of the anterior talofibular ligament
•
Talar tilt - assess for instability of the calcaneofibular ligament
•
External rotation - assess for instability of the syndesmosis
•
Syndesmotic squeeze test - assess for injury to the syndesmosis (distinguish medial and lateral
ankle sprains from a high ankle sprain)
•
Ottowa ankle rules help to determine the necessity of obtaining x-rays to rule out an ankle
fracture
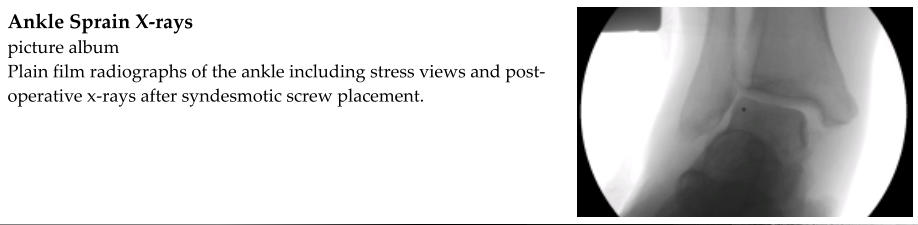
X-rays:
•
AP, lateral, oblique (mortise view) of ankle
•
Usually normal
•
Consider stress views if concernes about excessive talar tilt or other instability
•
Widening of the ankle mortise suggests syndesmotic injury
MRI:
•
Allows for visualization of soft tissue
•
Identifies occult fractures
•
May be obtained if there is concern for injury to the articular cartilage
•
May be obtained if there is concern for instability (excessive talar tilt, widening of the mortise)
•
Pre-operative planning in the case of an unstable ligament
Classification:
•
Location
o
Lateral
▪
Anterior talofibular ligament (most common)
▪
Calcaneofibular ligament
▪
Posterior talofibular ligament
o
Medial
▪
Deltoid ligament
•
Posterior tibiotalar ligament
•
Tibiocalcaneal ligament
•
Tibionavicular ligament
o
Syndesmosis (high ankle sprain)
▪
Anterior inferior tibiofibular ligament
▪
Posterior inferior tibiofibular ligament
▪
Interosseous membrane
•
Severity
o
Grade 1 - mild partial tear of the ligament without gross instability
o
Grade 2 - incomplete tear of the ligament, possibly with some laxity
o
Grade 3 - complete tear of the ligament with gross instability
Treatment:
•
The vast majority of ankle sprains are treated nonoperatively
•
Surgery may be considered if the fracture is unstable
o
Excessive laxity or talar tilt
o
Widening of the ankle mortise
•
Nonoperative
o
Immediate - RICE
▪
Rest
▪
Ice
▪
Compression
▪
Elevation
o
Phase 1 - immobilization
▪
not necessary for mild ankle sprains
▪
2-4 weeks depending on severity of sprain
▪
CAM walker boot or short leg cast
▪
bear weight as tolerated
▪
ice and elevation
o
Phase 2 - rehabilitation
▪
range-of-motion
▪
strengthening
▪
proprioception
o
Phase 3 - maintenance and return to play