









ACL Tear
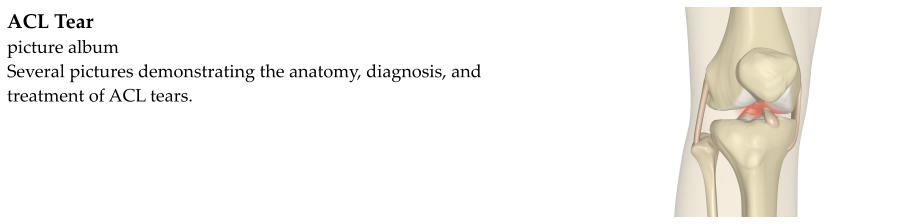
The knee joint is formed where the femur (the thigh bone) meets the tibia (the shin bone). Ligaments are tough,
band-like structures that hold bones together. The femur and tibia are held together by four main ligaments.
The ligaments on the sides of the knee are known as the collateral ligaments. They keep the knee from bending too
far to the side. The ligaments on the inside of the knee, within the joint, are known as the cruciate ligaments.
Cruciate means "cross-shaped." The cruciate ligaments cross one another in the knee. They help to stabilize the
knee by keeping the tibia from gliding too far forward or backward in relation to the femur. They also help with
rotational stability.
The anterior cruciate ligament, or ACL, keeps the tibia from gliding too far forward in relation to the femur. As
with any ligament, the ACL can be torn if too much force is applied to it. ACL tears are common in sports. They
are notorious for being non-contact injuries, meaning that they do not usually occur because of a blow to the knee.
Instead, they often occur as the result of a pivoting and twisting injury, a hyperextension injury, or during rapid
deceleration (meaning to come to a quick stop).
When the ACL tears, a sharp pain is felt within the knee joint. This may be accompanied by a pop and the knee
usually swells. Athletes are usually unable to continue competing after the injury.
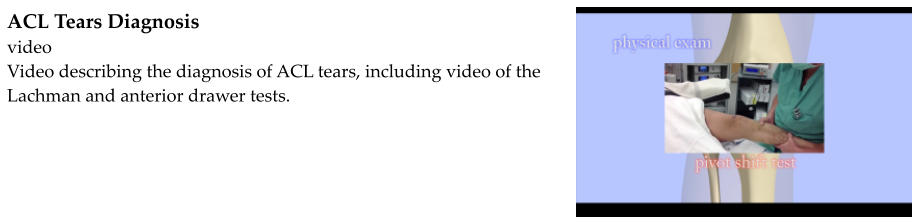
If an ACL tear is suspected the knee is examined. A few maneuvers have been described that test the ACL to
ensure that it is still intact and contributing to knee stability. They include Lachman's test and the anterior drawer
test which involve pulling forward on the tibia to see if it glides too far forward in relation to the femur. The pivot-
shift test is also utilized, but is usually difficult to perform because of pain.
X-rays are often obtained to rule out other injuries such as fractures and dislocations. But the ACL is not visible on
plain film x-rays.
Magnetic resonance imaging, or MRI, is the imaging test of choice for diagnosing ACL tears. The tear is usually
clearly visible on an MRI. MRIs are also helpful for distinguishing sprains and partial tears of the ACL from
complete tears. Other injuries often occur with the ACL tear which can be identified on an MRI as well, such as
meniscus tears and other ligament tears.
Initial treatment for an ACL tear is ice, elevation, and avoiding strenuous activity on the knee. Unfortunately, ACL
tears do not heal on their own. In order to restore the stability of the knee, especially in athletes, it is necessary to
surgically reconstruct the ACL with a graft. ACL reconstruction is recommended for younger, more active people.
For older, more sedentary people ACL reconstruction may not be worth doing, especially if osteoarthritis is already
present. This is a decision that should be made with the aid of a physician.
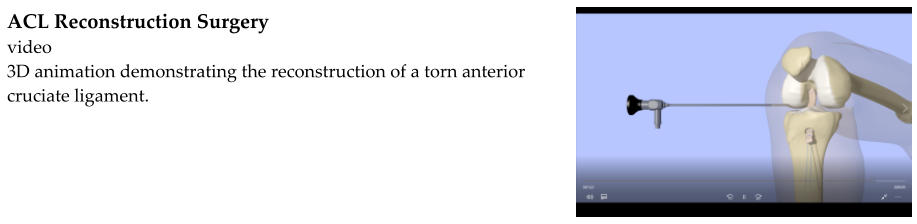
ACL reconstructions are usually done under general anesthesia, meaning that the person is put completely to
sleep. ACL reconstruction is done arthroscopically. Rather than making a large incision and opening up the joint
to reach the ACL, smaller incisions are made, just large enough to pass a small camera and instruments. A slender
scope is introduced into the knee to allow the surgeon to visualize the operative site. The torn ACL is removed.
Tunnels are then drilled in the femur and tibia. A graft is passed through the tunnels and takes the place of the
removed ACL. The graft is fixed in place and the incisions are closed.
The graft is a strong, thick band of tissue. It may be formed from tendons taken somewhere from the person's own
body. This is known as an autograft. Or it may be formed from tendons taken from a cadaver. This is known as an
allograft. Autografts and allografts each have their own benefits.
Rehabilitation following ACL reconstruction is very important. Physical therapists and trainers work with
orthopedic surgeons to put together an appropriate program. For the first few weeks, physical therapy focuses on
protecting the graft and restoring range-of-motion. After a few weeks, the graft will have healed into the bone
enough to begin strengthening the muscles surrounding the knee. As the strength and stability of the knee
improve, running, cutting, jumping, and sport-specific drills can be incorporated into therapy. Full recovery after
an ACL reconstruction usually takes between 6 and 12 months.